I attended the first conference of its kind this past weekend ... the American Society of Clinical Oncology (ASCO)'s Cancer Survivorship Symposium. This meeting was a collaboration between oncologists and primary care physicians in addressing the myriad of needs of a cancer survivor. There were close to 1,000 people attending the conference, the bulk being in the medical profession.
I've been asked ... why would you attend such a meeting? You are not a "survivor." You are going to die of this disease.
To be honest, I've long struggled with the use of the word "survivor" as it does indicate that an event that is survived is in the past. Many with cancer also struggle with the word as well. As an teacher of English as a second/foreign language, I wonder about how much time should be spent on the semantics of the concept, but then my tired brain pulled an Elsa and I just "let it go."
I've been asked ... why would you attend such a meeting? You are not a "survivor." You are going to die of this disease.
To be honest, I've long struggled with the use of the word "survivor" as it does indicate that an event that is survived is in the past. Many with cancer also struggle with the word as well. As an teacher of English as a second/foreign language, I wonder about how much time should be spent on the semantics of the concept, but then my tired brain pulled an Elsa and I just "let it go."
The National Coalition for Cancer Survivorship (NCCS) defines a cancer survivor as anyone with a history of cancer, from the time of diagnosis and for the remainder of life, whether that is days or decades." This is the definition that was used throughout the conference.
There is much talk in the metastatic breast cancer community to push metastatic breast cancer into the "chronic disease" classification. Once again, I have struggled with that concept, but after this conference, I better understand what that means.
There is much talk in the metastatic breast cancer community to push metastatic breast cancer into the "chronic disease" classification. Once again, I have struggled with that concept, but after this conference, I better understand what that means.
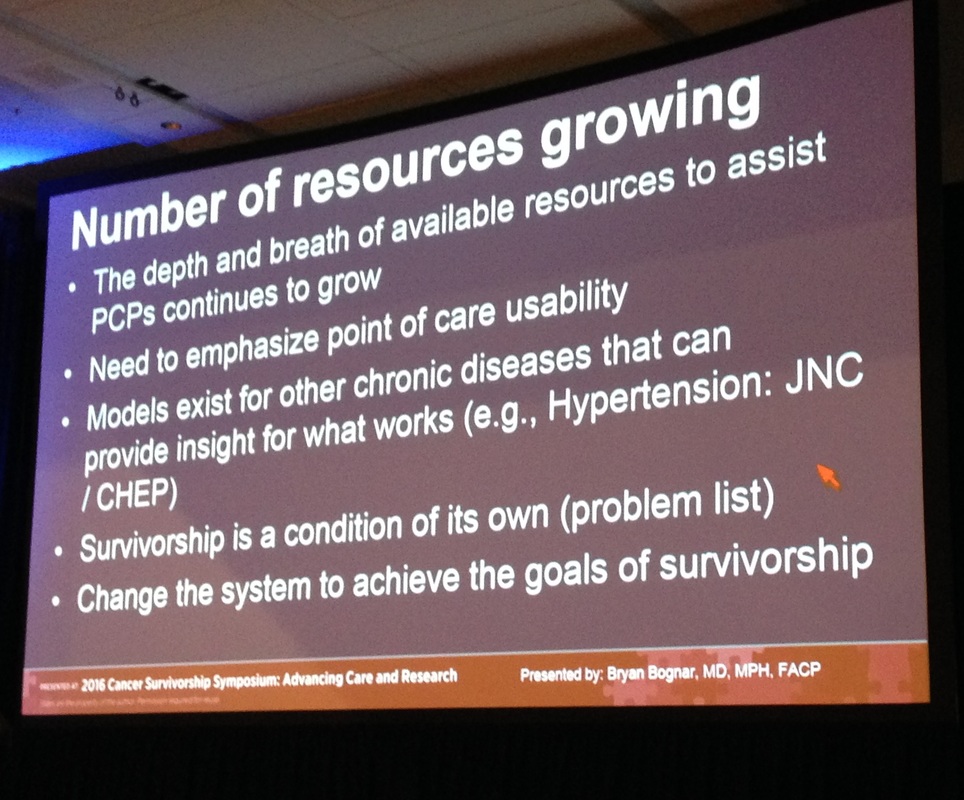
Survivorship is a condition of its own, with its own problem list.
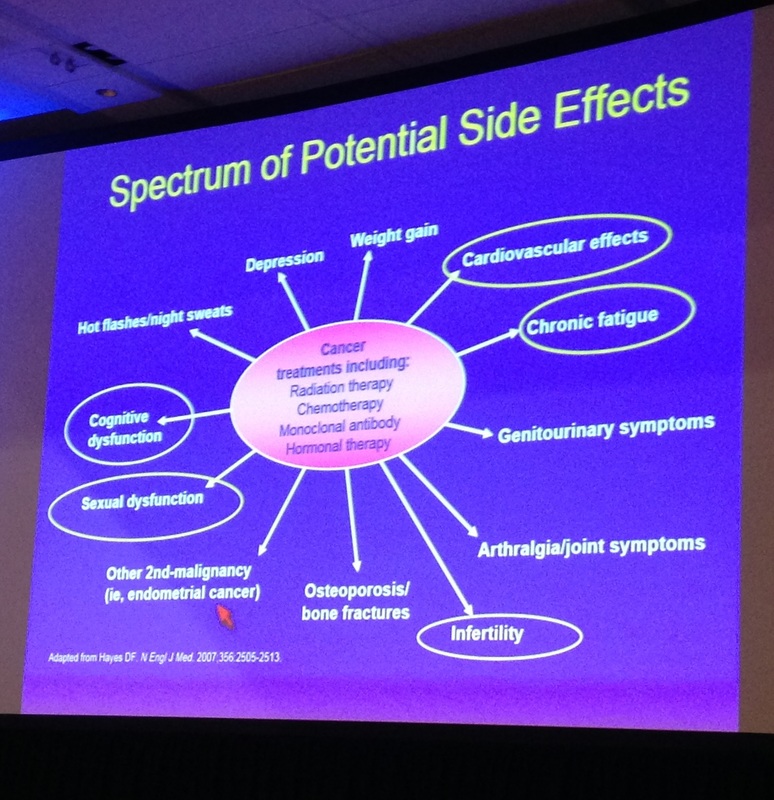
(The circled items are those that were addressed at the conference.)
If metastatic breast cancer is to be considered a chronic condition, then, just as it's important to understand the impact that a primary cancer has on someone for the rest of their lives, it is also important to understand the myriad of conditions that accompany a metastatic diagnosis.
Emphasis was made on how other conditions already classified as chronic have the appropriate follow-up care plans in place and that re-invention wasn't necessary, but that using those conditions as models would expedite the process. The general consensus is that every cancer patient should receive a Cancer Survivorship Plan upon completion of their treatment and that this plan should not be dependent upon the patient pulling it together.
Two of the saddest statements made at the conference were:
"Early detection of recurrence does not make sense when no effective therapy is available." and "Not everyone in this country can afford to have cancer."
These are volatile statements. I understand the premise of not testing for recurring disease when there are no symptoms, but if a disease can be controlled for a longer period of time using less toxic therapies, then the earlier that recurrent disease can be found seems better. Doctors feel challenged to know what type of follow-up is needed, especially for those survivors of childhood cancers. The general consensus was that scans or blood tumor markers should not be used unless the patient presents with symptoms
This question came up over and over ... who is going to pay for all this followup needed for a cancer patient? There was never a satisfactory answer from anyone.
EVERYONE wants better follow-up and care. However, given the current condition of health care provision in the United States, this can be difficult to finance. It's not enough to have a moonshot cure for cancer if there isn't an infrastructure in place to support all those cured people. The "cure" can come with a high cost at the physical, psychological and financial levels.
There were many talks and presentation on the value of physical movement and proper nutrition for risk reduction. Those who called these two "whole patient" approaches as preventive measures were consistently challenged. Risk reduction is not the same thing as prevention and risk reduction is not a guarantee.
I was able to ask questions in two of the sessions, thus getting metastatic disease into the discussion. While metastatic disease was not the focus of this symposium, it is important that if we are going to push metastatic disease into the chronic category, then the needs and concerns of metastatic patients need to be addressed as well.
Both of my questions were well received and applauded. My first question was regarding the use of "risk reduction vs prevention" and the presenting doctor apologized and corrected her terminology. My second question was more of a comment in the need for more effective treatments that didn't cause such devastating side effects, whether immediate of late-term in treating cancer. I said that we should not accept it as "normal" that someone who survived a childhood cancer should not have to deal with the aftermath of the disease and treatment decades later.
One of the most appalling things that happened, though, was when a PhD (and co-author of a best selling nutrition book) gave me three referrals to alternative practitioners to handle my metastatic disease. She even used the term "cure your disease" when talking about one of them because he cured someone else's Stage III disease. I told her that there was no cure for metastatic disease and that anyone who claimed such a thing was a fraud. She corrected herself and talked about his helping me live a long time with the disease.
Sigh. I accepted the three names and I immediately looked them up. I'm always wanting to know who is following whom and why.
This is what is appalling. One of her referrals was arrested in July 2015 for practicing without a license, giving expired medications and giving a bag of dirt as a treatment protocol for a woman with metastatic breast cancer. There are no records of his having any education of any kind beyond high school, yet he is touting himself as a chemist and doctor ... and as the one who has the cure for cancer.
If you are going to take the time to seek someone out to give a referral, it would be good to know everything about that referral and whether or not you want your name to be associated with that referral. Needless to say, I'm not interested in any of the referrals. I am not interested in anything she has to say. She has lost all credibility with me.
I am interested in evidenced based protocol, not woo-woo wishful thinking.
I learned a lot. I'm still processing. I have a long way to go. I networked like crazy, gained access to a lot of resources, talked to a lot of people involved in both advocacy and research and I came home absolutely exhausted.
There's so much we know, yet so much we don't know.
"Early detection of recurrence does not make sense when no effective therapy is available." and "Not everyone in this country can afford to have cancer."
These are volatile statements. I understand the premise of not testing for recurring disease when there are no symptoms, but if a disease can be controlled for a longer period of time using less toxic therapies, then the earlier that recurrent disease can be found seems better. Doctors feel challenged to know what type of follow-up is needed, especially for those survivors of childhood cancers. The general consensus was that scans or blood tumor markers should not be used unless the patient presents with symptoms
This question came up over and over ... who is going to pay for all this followup needed for a cancer patient? There was never a satisfactory answer from anyone.
EVERYONE wants better follow-up and care. However, given the current condition of health care provision in the United States, this can be difficult to finance. It's not enough to have a moonshot cure for cancer if there isn't an infrastructure in place to support all those cured people. The "cure" can come with a high cost at the physical, psychological and financial levels.
There were many talks and presentation on the value of physical movement and proper nutrition for risk reduction. Those who called these two "whole patient" approaches as preventive measures were consistently challenged. Risk reduction is not the same thing as prevention and risk reduction is not a guarantee.
I was able to ask questions in two of the sessions, thus getting metastatic disease into the discussion. While metastatic disease was not the focus of this symposium, it is important that if we are going to push metastatic disease into the chronic category, then the needs and concerns of metastatic patients need to be addressed as well.
Both of my questions were well received and applauded. My first question was regarding the use of "risk reduction vs prevention" and the presenting doctor apologized and corrected her terminology. My second question was more of a comment in the need for more effective treatments that didn't cause such devastating side effects, whether immediate of late-term in treating cancer. I said that we should not accept it as "normal" that someone who survived a childhood cancer should not have to deal with the aftermath of the disease and treatment decades later.
One of the most appalling things that happened, though, was when a PhD (and co-author of a best selling nutrition book) gave me three referrals to alternative practitioners to handle my metastatic disease. She even used the term "cure your disease" when talking about one of them because he cured someone else's Stage III disease. I told her that there was no cure for metastatic disease and that anyone who claimed such a thing was a fraud. She corrected herself and talked about his helping me live a long time with the disease.
Sigh. I accepted the three names and I immediately looked them up. I'm always wanting to know who is following whom and why.
This is what is appalling. One of her referrals was arrested in July 2015 for practicing without a license, giving expired medications and giving a bag of dirt as a treatment protocol for a woman with metastatic breast cancer. There are no records of his having any education of any kind beyond high school, yet he is touting himself as a chemist and doctor ... and as the one who has the cure for cancer.
If you are going to take the time to seek someone out to give a referral, it would be good to know everything about that referral and whether or not you want your name to be associated with that referral. Needless to say, I'm not interested in any of the referrals. I am not interested in anything she has to say. She has lost all credibility with me.
I am interested in evidenced based protocol, not woo-woo wishful thinking.
I learned a lot. I'm still processing. I have a long way to go. I networked like crazy, gained access to a lot of resources, talked to a lot of people involved in both advocacy and research and I came home absolutely exhausted.
There's so much we know, yet so much we don't know.

 RSS Feed
RSS Feed
